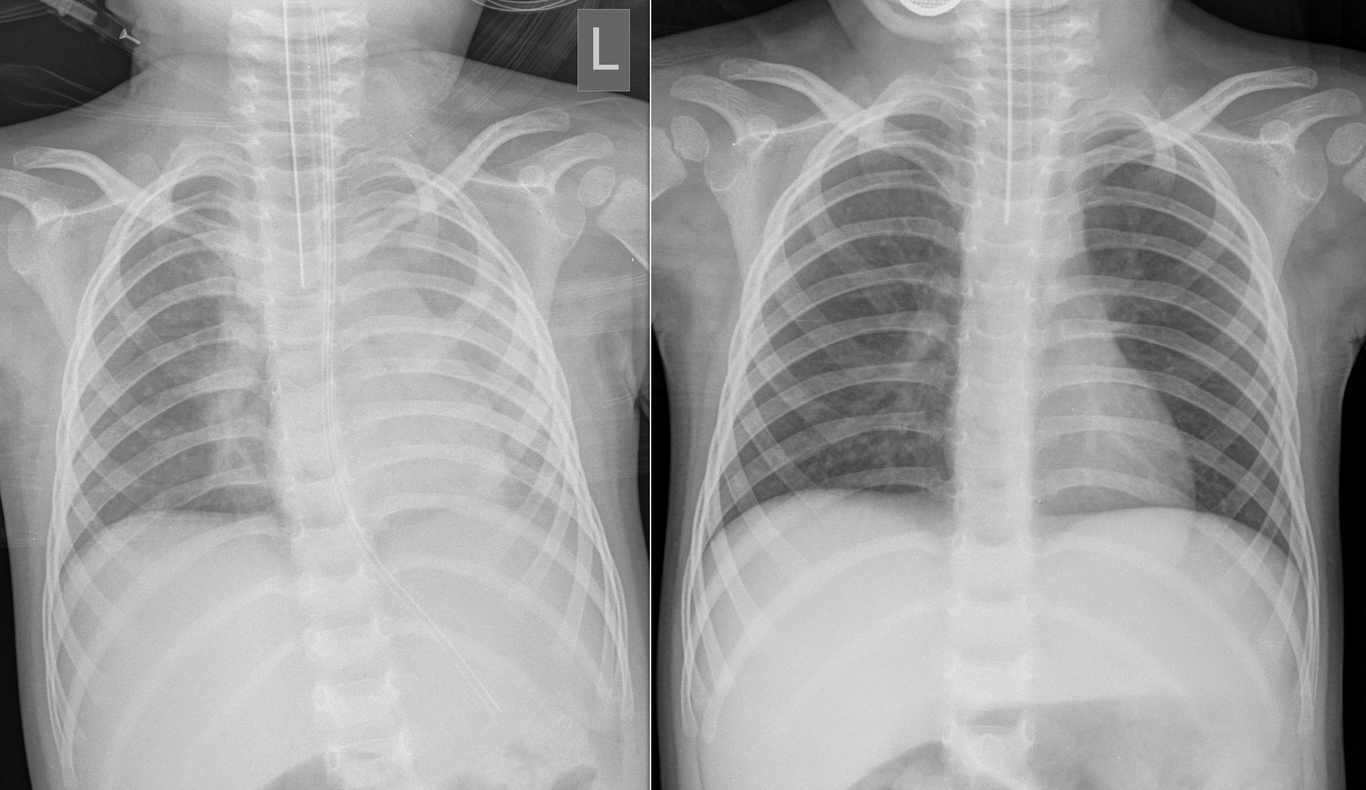
Real-time ultrasound guided segmental bronchoscopic insufflation in a Tay-Sachs patient with atelectasisMatej Šapina, MD, PhD1,2,3*, Bojana Olujić, MD1,2, Tihana Nađ, MD1,2, Hrvoje Vinković, MD1,2, Zdravka Krivdić Dupan, MD1,2, Nikolina Hamidović, MD1, Mia Damašek, MD1,2, Krešimir Milas, MD1, Željko Zubčić, MD, PhD1,2, and Ivan Erić, MD, PhD1,21University hospital center Osijek, 31000 Osijek, Croatia2Medical faculty Osijek, 31000 Osijek, Croatia3Faculty of dental medicine and health Osijek, 31000 Osijek, Croatia*Corresponding author: [email protected]: +385 31 512 279Keywords: bronchoscopy, atelectasis, Tay-Sachs diseaseIntroductionTo the Editor,Atelectasis is the collapse of lung tissue and is a common problem in patients suffering from severe neurological diseases. Treatment depends on the underlying cause, and ranges from respiratory physiotherapy, mucus clearance methods, and in some cases bronchoscopic interventions. If left untreated recurrent infections may occur, along with impaired gas exchange and in the long run fibrosis of the affected area1.A female patient at the age of 3 years with Tay-Sachs disease and consequent severe global psychomotor delay and epilepsy was initially admitted due to a respiratory infection to the neuropediatric department, where she developed an epileptic status and desaturation, prompting a transfer to the Intensive Care Unit. The refractory epileptic status resolved only with several antiepileptics, which lead to intubation requiring invasive mechanical ventilation, after which the patient stabilized.An attempt to reduce sedation the next day resulted in repeated seizures. On the third day, inflammatory parameters increased, with a radiological finding suggestive of pneumonia and a large left atelectasis confirmed by ultrasound. Antibiotics were empirically started, and Moraxella catarrhalis and Adenovirus in the respiratory tract were obtained in the cultures.Lung ultrasound showed a large consolidation in the dorsal upper two thirds of the left hemithorax. Due to the size of the atelectasis, we decided to perform bedside bronchoscopy.A single use paediatric flexible bronchoscope (Ambu® aScope™ 5 Broncho) was introduced through the ETT. The tracheobronchial morphology did not show any obstructions. We applied our recently published modified segmental insufflation technique, however without the use of surfactant2.First, a bronchoalveolar lavage was performed for microbiological and cytological analysis, followed by ultrasound guided bronchoscopic treatment of the affected area. The patient was positioned on the right lateral decubitus position. As described previously, a cuff pressure manometer (AG Cuffill Cuff) and a 50 ml syringe were attached to a three-way stopcock connected to the bronchoscope’s working channel. Pressure controlled segmental insufflation of the lingula and upper lobe was performed directly observing an aeration of the atelectatic areas on the ultrasound with no complications.Subsequent ultrasound monitoring resulted in total expansion of the affected lung and resolution of inflammation, confirmed radiologically (Figure 1.). The patient could be safely extubated and transferred to the wards. No reoccurrence of atelectasis was observed.ConclusionThe treatment of pediatric atelectasis poses a challenge, with limited approaches available and a lack of evidence-based guidelines to guide clinical decision-making. A question that remains to be answered is not only the mode of treatment, but timing. Even with bronchoscopic treatment, different methods exist. In obstructive atelectasis, the approach is simple - to eliminate the obstruction, however, nonobstructive atelectasis remain challenging. Bronchoscopic lung insufflation technique has been explored in adults, with limited cases reported in children3. Several case reports utilized pressure-controlled insufflation with or without surfactant in long standing atelectasis as an add on treatment2; 4.We believe that patients with severe neurological diseases require special attention regarding their susceptibility for developing atelectasis5. Our approach is early bronchoscopic pressure-controlled insufflation in non-obstructive atelectasis. Depending on the duration, we additionally instill surfactant in long standing ones.Ultrasound is recently being used in lung recruitment maneuvers to monitor lung expansion, however, it was only recently reported to be utilized for segmental insufflation monitoring in a spinal muscular atrophy type I patient4. However, to our best knowledge, our case report is the first successful use on a Tay-Sachs patient using real time ultrasound monitoring during pressure-controlled segmental bronchoscopic insufflation. The benefits of ultrasound guidance is the direct visualisation of lung expansion reducing the need for fluoroscopic radiation exposure of visualisation and further monitoring. Besides it increases the safety of the procedure allowing for detection of development of pneumothorax.In conclusion, pressure controlled real-time ultrasound guided bronchoscopic segmental insufflation, with its low-cost, lightweight, and flexible setup, seems to be a safe and promising new modality for treatment of non-obstructive atelectasis, especially in children requiring complex care.FIGURESFigure 1. On the left a large left sided atelectasis can be seen causing the mediastinal shift. On the right complete regression of the atelectasis is observed before extubatingReferences1. Ogake S, Bellinger C. 2020. Role of bronchoscopy in atelectasis. Clinical Pulmonary Medicine. 27(1):30-32.2. Šapina M, Olujic B, Nađ T, Vinkovic H, Dupan ZK, Bartulovic I, Milas K, Kos M, Divkovic D, Zubčić Z. 2023. Bronchoscopic treatment of pediatric atelectasis: A modified segmental insufflation‐surfactant instillation technique. Pediatric Pulmonology.3. Abu‐Hasan MN, Chesrown SE, Jantz MA. 2013. Successful use of bronchoscopic lung insufflation to treat left lung atelectasis. Pediatric Pulmonology. 48(3):306-309.4. Esteban IA, Osona B, Ballestín AS, Rubio CC, de Mendiola JMFP, Gómez VA, López ME, Vicente JCDC. 2024. Bronchoscopic segmental alveolar recruitment in a patient with spinal muscular atrophy and massive atelectasis. Pediatric pulmonology.5. St‐Laurent A, Zysman‐Colman Z, Zielinski D. 2022. Respiratory prehabilitation in pediatric anesthesia in children with muscular and neurologic disease. Pediatric Anesthesia. 32(2):228-236.