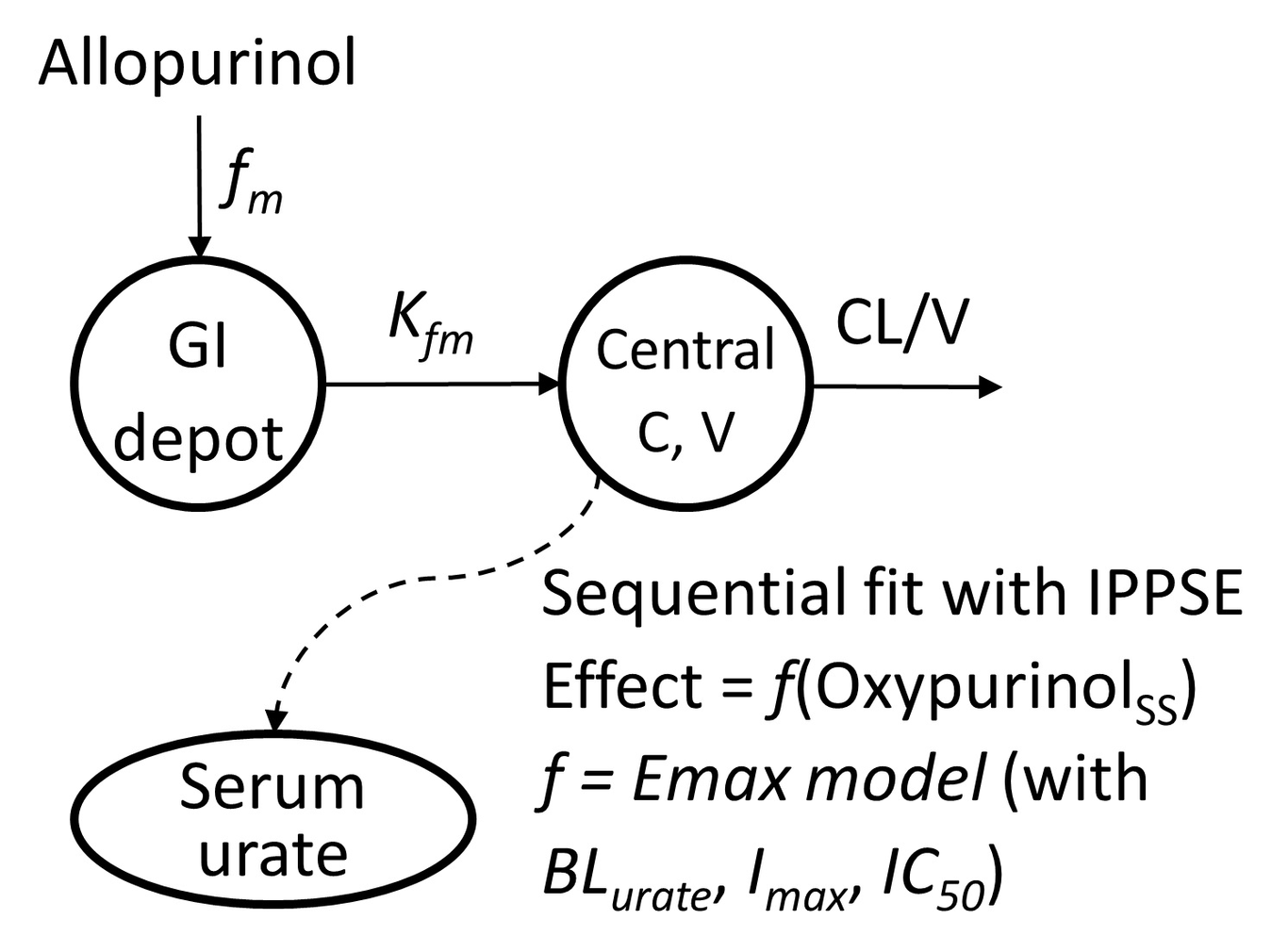
Aim: Quantify identifiable sources of variability, including key pharmacogenetic variants in oxypurinol pharmacokinetics and their pharmacodynamic effect on serum urate. Methods: Hmong participants (n=34) received 100 mg allopurinol twice daily for 7 days followed by 150 mg allopurinol twice daily for 7 days. Serum urates (SU) were obtained pre- and post-allopurinol. Serum oxypurinol concentrations were obtained at times 0, 2, 4, and 6 hours after the last dose. A sequential population pharmacokinetic pharmacodynamics (PKPD) analysis with non-linear mixed-effects modeling evaluated the impact of anthropometrics, concomitant medications, and genetic variants on oxypurinol PKPD parameters. Allopurinol maintenance dose to achieve target SU was simulated based on the final PKPD model. Results: A one-compartment model with first order absorption and elimination best described the oxypurinol concentration-time data. Inhibitory of SU by oxypurinol was described with a direct inhibitory Emax model using steady-state oxypurinol concentrations. Fat-free body mass, estimated creatinine clearance and SLC22A12 rs505802 genotype were found to predict differences in oxypurinol clearance. Oxypurinol concentration required to inhibit 50% of xanthine dehydrogenase activity was affected by PDZK1 rs12129861 genotype. Most individuals with both PDZK1 rs12129861 AA and SLC22A12 rs505802 CC genotypes achieve target SU with allopurinol below the maximum dose, regardless of renal function and body mass. In contrast, individuals with both PDZK1 rs12129861 GG and SLC22A12 rs505802 TT genotypes would require more than the maximum dose, thus alternative medications. Conclusion: The proposed allopurinol dosing guide uses individuals’ fat-free mass, renal function, and SLC22A12 rs505802 and PDZK1 rs12129861 genotypes to achieve target SU.