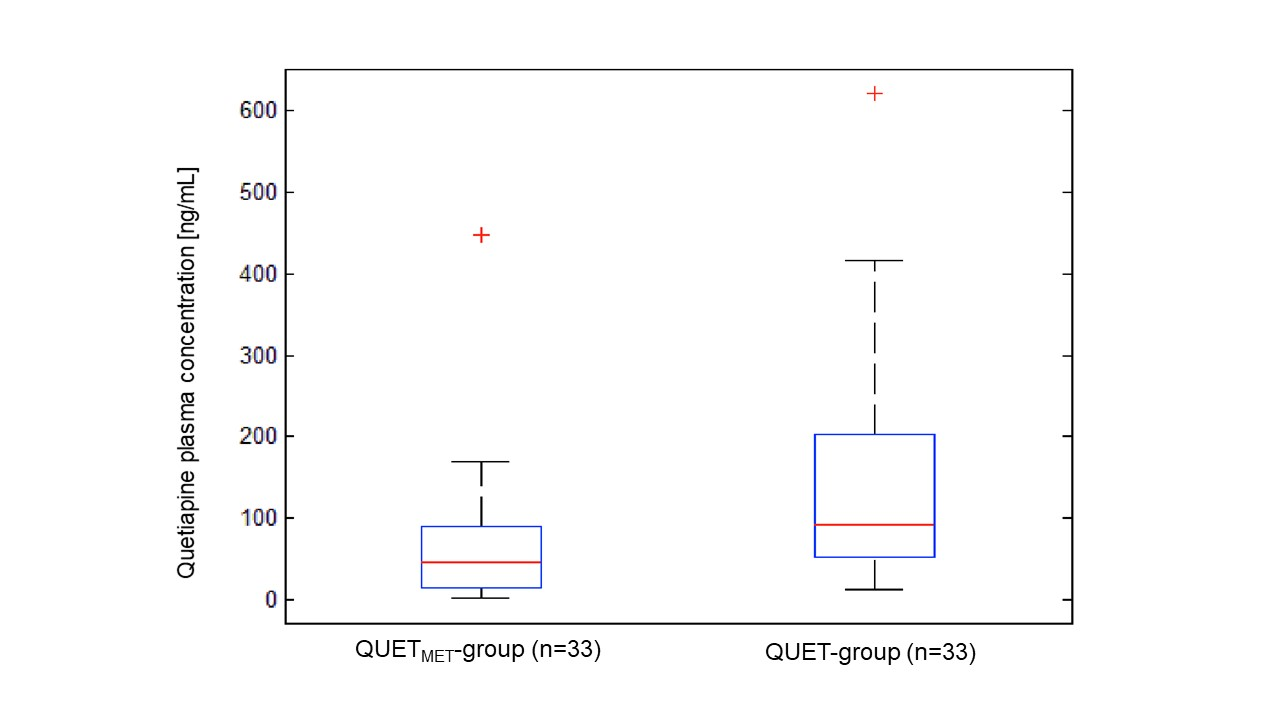
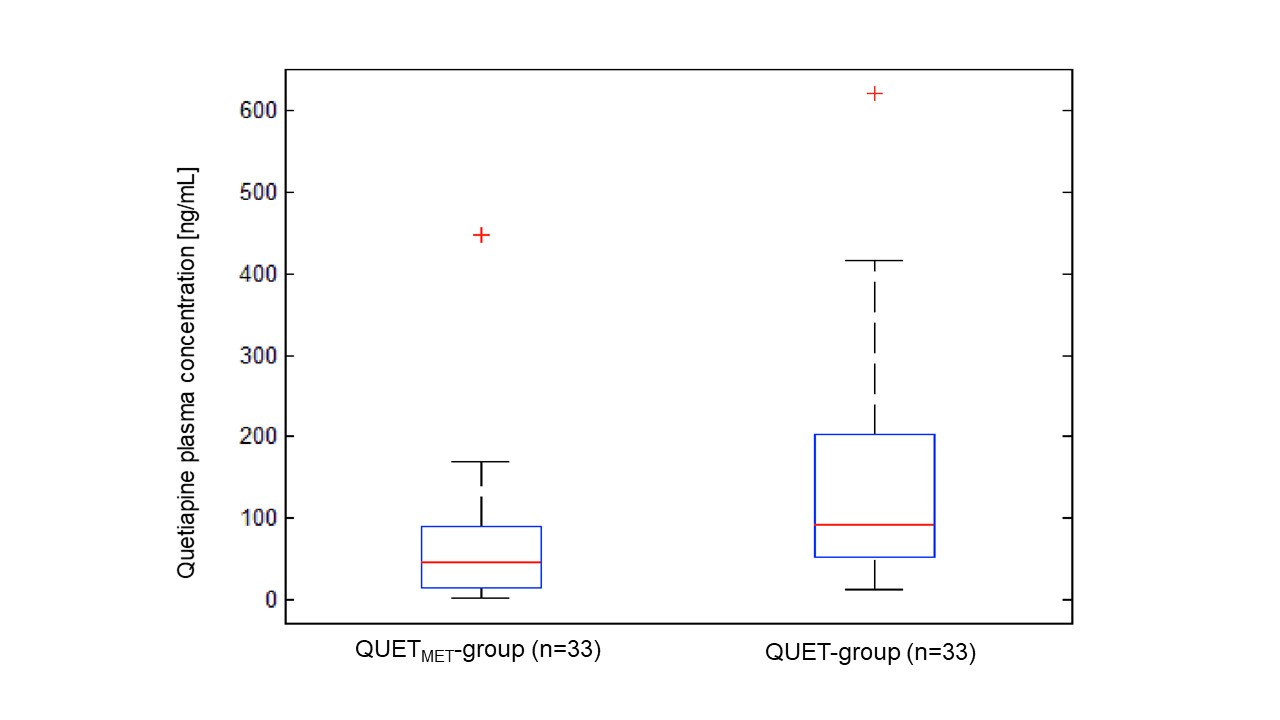
Objective: Metamizole is quite an old drug with analgesic, antipyretic and spasmolytic properties. Recent findings have shown that it may induce several cytochrome P450 enzymes, especially CYP3A4 and CYP2B6. The clinical relevance of these properties is uncertain. We aimed to unravel potential pharmacokinetic interactions between metamizole and the CYP3A4 substrate quetiapine. Methods: Plasma concentrations of quetiapine from a large therapeutic drug monitoring database were analyzed. Two groups of 33 patients, either receiving quetiapine as a monotherapy (without CYP modulating co-medications) or with concomitantly applied metamizole were compared addressing a potential impact of metamizole on the metabolism of quetiapine being reflected in differences of plasma concentrations of quetiapine and dose-adjusted plasma concentrations (C/D). Results: Patients co-medicated with metamizole showed significantly lower plasma concentrations of quetiapine (median 45.2 ng/mL, Q1=15.5; Q3=90.5 vs. 92.0 ng/mL, Q1=52.3; Q3=203.8, p=0.003). Accordingly, plasma concentrations of quetiapine in the control group were more than twice of those in the metamizole group (+103% higher). The dose-adjusted plasma concentrations were 69 % lower in the co-medication group (p=0.001). Conclusions: The combination of metamizole and quetiapine leads to significantly lower drug concentrations of quetiapine, most likely via an induction of cytochrome P450 CYP3A4 by metamizole. Clinicians have to consider the risk of adverse drug reactions, especially treatment failure under quetiapine when adding metamizole.