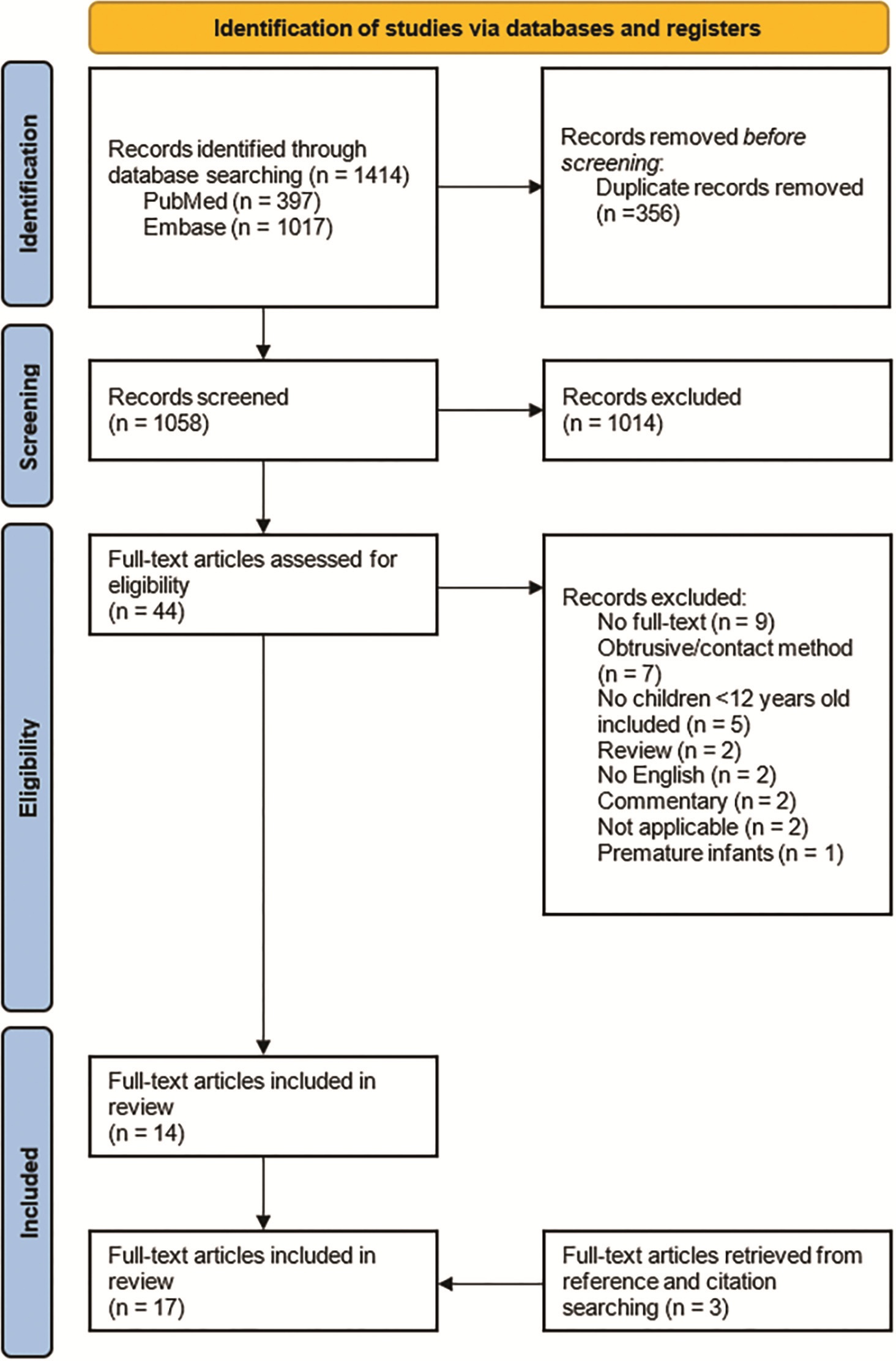
Pediatric sleep-related breathing disorders, or sleep-disordered breathing (SDB), cover a range of conditions including obstructive sleep apnea (OSA), central sleep apnea (CSA), sleep-related hypoventilation disorders, and sleep-related hypoxemia disorder. Pediatric SDB is often underdiagnosed, potentially due to difficulties associated with performing the gold standard polysomnography (PSG) in children. This scoping review aims to: 1) provide an overview of the studies reporting on safe, noncontact monitoring of respiration in young children; 2) describe the accuracy of these techniques, and 3) highlight their respective advantages and limitations. PubMed and EMBASE were searched for studies researching techniques in children <12 years old. Both quantitative data and the quality of the studies were analyzed. The evaluation of study quality was conducted using the QUADAS-2 tool. A total of 17 studies were included. Techniques could be grouped into bed-based methods, ultra-wideband (UWB) radar, Doppler radar, video, infrared (IR) cameras, garment-embedded sensors, and sound analysis. Most either measured respiratory rate (RR) or detected apneas; five aimed to do both. Noncontact sleep monitoring techniques are safe, but accuracy data of these techniques is limited, and large heterogeneity exists regarding study quality and stage. Motion artifacts affect accuracies of apnea detection. Sleep respiration analysis could benefit from sleep stage classification and breathing sound analysis. Further research is crucial to facilitate easily accessible and safe non-contact methods for respiration monitoring in a home setting.