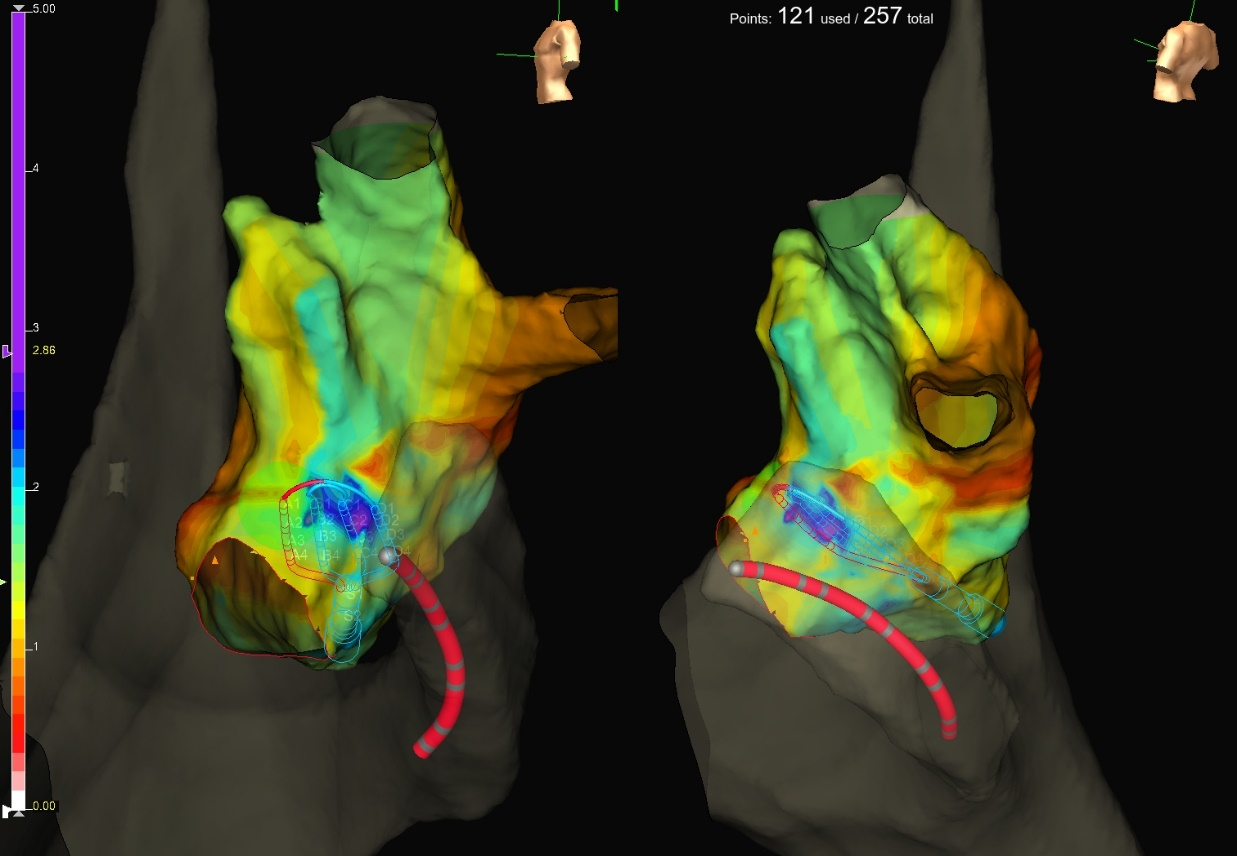
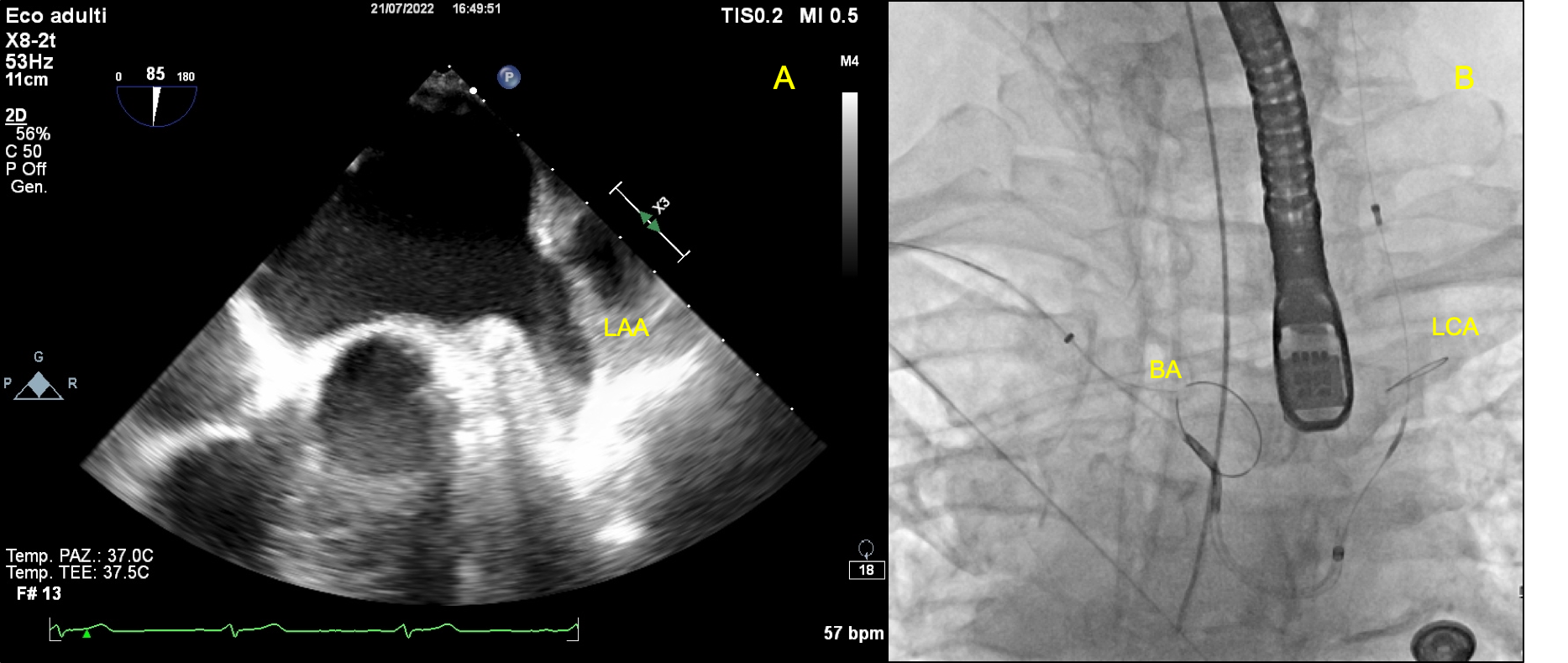
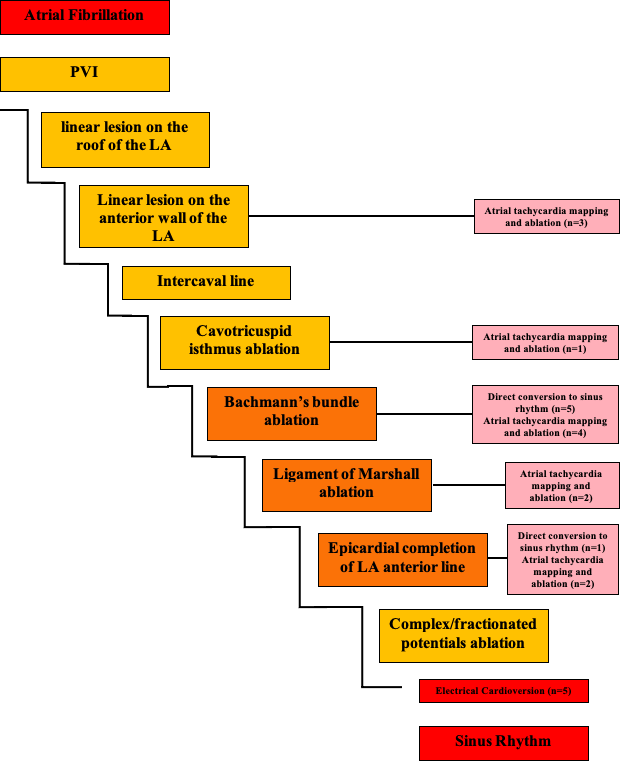
Background: Outcomes of catheter ablation (CA) among patients with non-paroxysmal atrial fibrillation (AF) are largely disappointing. Objective: We sought to evaluate the feasibility, effectiveness, and safety of a single-stage stepwise endo-/epicardial approach in patients with persistent/longstanding-persistent AF. Methods: We enrolled 25 consecutive patients with symptomatic persistent (n=4) or longstanding-persistent (n=21) AF and at least one prior endocardial procedure, who underwent CA using an endo-/epicardial approach. Our anatomical stepwise protocol included multiple endocardial as well as epicardial (Bachmann’s bundle [BB] and ligament of Marshall ablations) components, and entailed ablation of atrial tachycardias emerging during the procedure. The primary outcome was freedom from any AF/atrial tachycardia episode after a 3-month blanking period. The secondary outcome was patients’ symptom status during follow-up. Results: The stepwise endo-/epicardial approach allowed sinus rhythm restoration in 72% of patients, either directly (n=6, 24%) or after AF organization into atrial tachycardia (n=12, 48%). BB’s ablation was commonly implicated in arrhythmia termination. After a median follow-up of 266 days (interquartile range, 96 days), survival free from AF/atrial tachycardia was 88%. Antiarrhythmic drugs could be discontinued in 22 patients (88%). As compared to baseline, more patients were asymptomatic at 9-month follow-up (0% vs- 56%, p=0.02). Five patients (20%) developed mild medical complications, whereas one subject (4%) had severe kidney injury requiring dialysis. Conclusion: a single-stage endo-/epicardial CA resulted in favorable rhythm and symptom outcomes in a cohort of patients with symptomatic persistent/longstanding-persistent AF and one or more prior endocardial procedures. Epicardial ablation of BB was commonly implicated in procedural success.