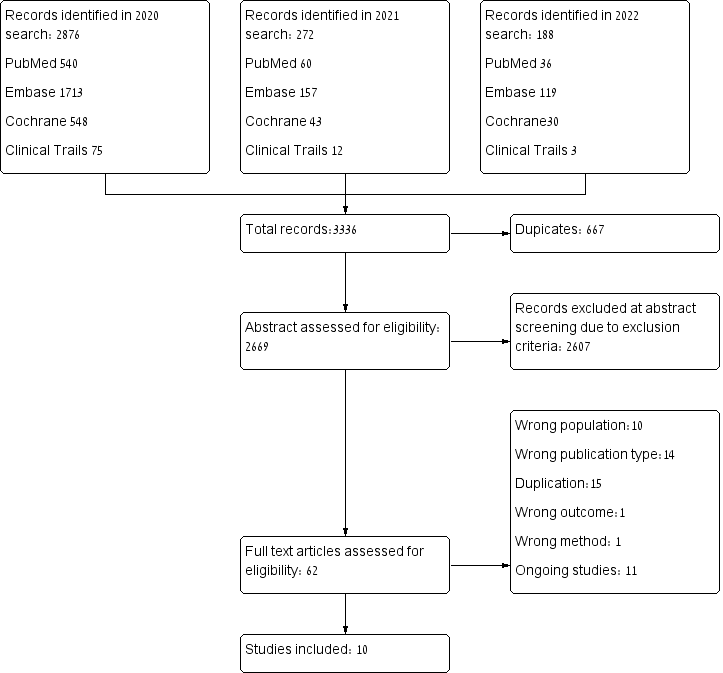
ABSTRACT Background: Obstetrical complications involving uteroplacental insufficiency associated disorders, such as preeclampsia, intrauterine growth restriction, and obstetric antiphospholipid syndrome, share pathophysiology and risk factors with cardiovascular diseases treated with statins. Objective: To evaluate associations of statin treatment with pregnancy prolongation, and neonatal and maternal morbidity, among women with uteroplacental insufficiency disorders. Search Strategy: Electronic databases including PubMed, Medline, Embase, Clinical Trials Registry Clinicaltrials.gov, and The Cochrane Library were searched from inception to January 2022. Selection Criteria: Cohort studies and randomized controlled trials (RCTs) Data collection and analysis: Pooled odds ratios were calculated using a random-effects model; meta-regression was utilized when applicable. Main Results: The analysis included ten studies describing 1391 women with uteroplacental insufficiency-associated disorders: 703 treated with pravastatin and 688 not treated with statins. Women who received pravastatin showed significant prolongation of pregnancy (mean difference 0.44 weeks, 95%CI:0.01-0.87, p=0.04, I2=96%) and less neonatal critical care unit admission (OR=0.42, 95%CI: 0.23-0.75, p=0.004, I2=25%). Trends were observed toward a decrease in preeclampsia diagnoses (OR=0.51, 95%CI:0.25–105, p=0.07, I=44%), and perinatal death (OR=0.32, 95%CI:0.09-1.13, p=0.08, I2=54%) and an increase in birth weight (mean difference=102 grams, 95%CI: -14–212, p=0.08, I2=96%). A meta-regression analysis revealed associations between earlier gestational age at initiation of pravastatin treatment to lower risk for development of preeclampsia (R2=1) and between longer duration of pravastatin treatment to lower rate of NICU admission (R2=0.33). No dose-response effect was demonstrated. Conclusions: Pravastatin treatment in pregnancies with high risk for developing uteroplacental insufficiency disorders may prolong pregnancy duration and improve neonatal outcomes.