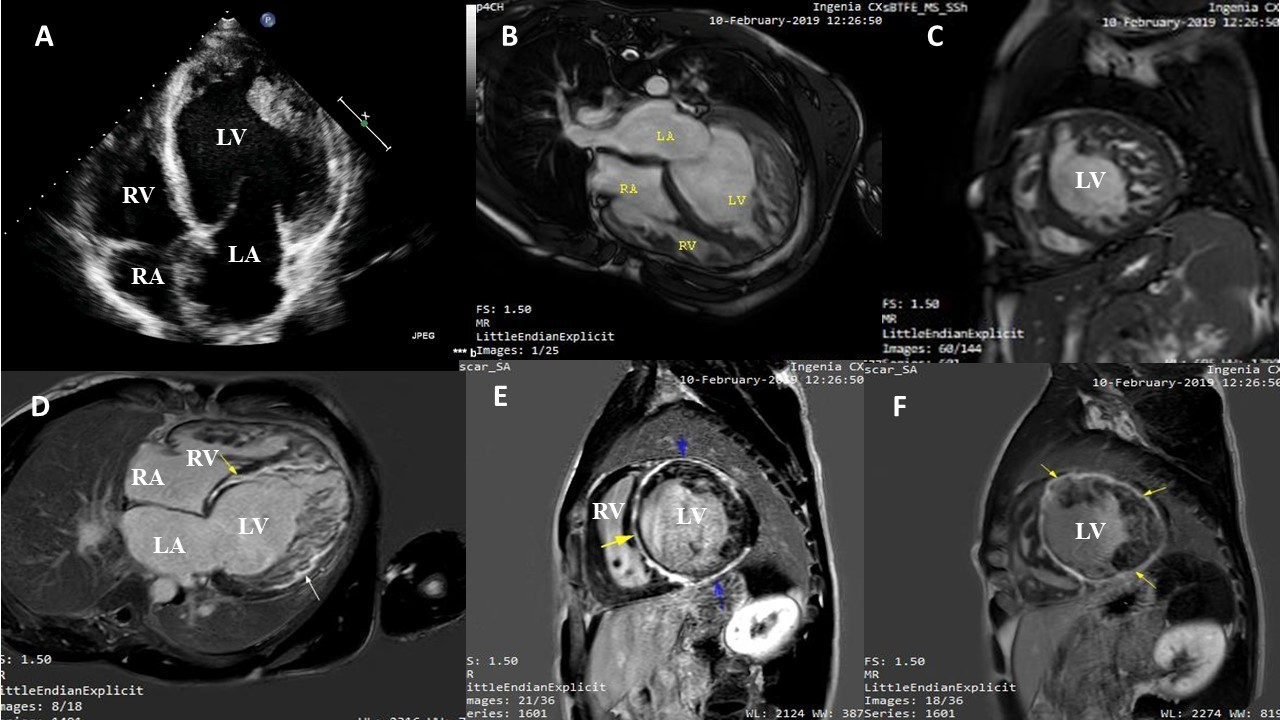
Myocardial non-compaction (NC) is a rare genetically heterogeneous cardiomyopathy which is characterized by excessively prominent ventricular trabeculations with deep intertrabecular recesses. It is commonly believed to be due to an intrauterine arrest of the endomyocardial morphogenesis. Left ventricle (LV) is the usual site of affection, but very rarely right ventricular (RV) or both ventricles may be involved. It can be isolated or associated with other cardiac diseases or neuromuscular disorders. It has a wide spectrum of clinical manifestations that range from asymptomatic status, progressive ventricular dysfunction, arrhythmias and congestive heart failure that have been found to be associated with myocardial fibrosis. Cardiac Magnetic resonance (CMR) is the gold standard non-invasive modality for the diagnosis of cardiomyopathies. In NC cases, late gadolinium enhancement (LGE) of the trabeculated layer or mild fibrosis of the compacted layer was previously described in the literature, however extensive fibrosis in the compacted layer only with no fibrosis at the trabeculated layer was not described before. We report a male patient presented with heart failure symptoms, echocardiogram showed severe LV and RV systolic dysfunction with prominent bi-ventricular trabeculations. CMR confirmed the diagnosis of bi-ventricular non-compaction with peculiar pattern extensive fibrosis of the compacted layer of LV in LGE. To the best of our knowledge, our case is the first case to report extensive fibrosis in the compacted layer only with no fibrosis at the trabeculated layer.