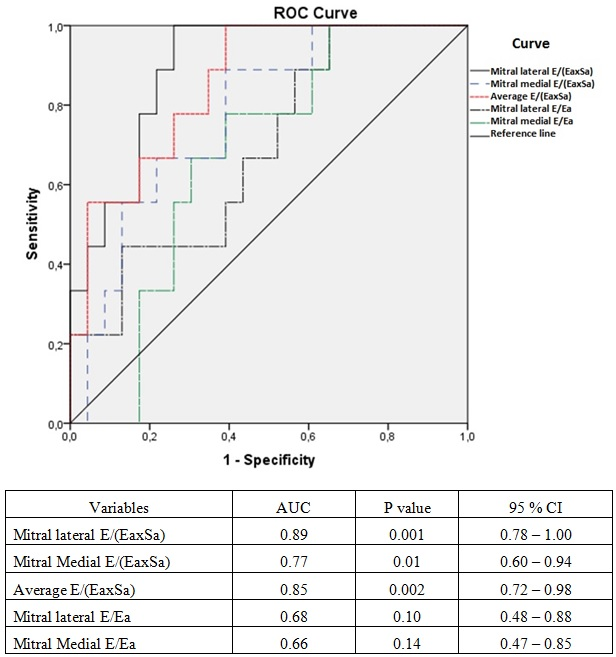
Objective:Identification of patients who are nonresponders to cardiac resynchronization therapy (CRT) with the use of simple and objective parameters may be helpful in tailoring treatment. The aim of this study is to investigate whether E/(Ea×Sa) could be a predictor of CRT nonresponders (E=early diastolic transmitral velocity, Ea=early diastolic mitral annular velocity, Sa=systolic mitral annular velocity). Methods:In total, 53 heart failure patients were evaluated for this study, and 33 patients were included according to the study criteria. Before and six months after CRT-D(CRT with a defibrillator) implantation, E, Ea, and Sa were determined at the medial and lateral mitral annular sites, and the average values were obtained. E/(Ea×Sa) was calculated (medial, lateral, average). The patients were followed for six months to monitor their CRT response. A responder was defined as a patient with a reduction in end-systolic volume of <15% and an increase in six-minute walking distance of 50 meters. Results:At a six-month follow-up, 24(72.7%) of the 33 patients responded to CRT. At the six-month follow-up, in the responder group, the E/Ea ratio, lateral mitral, and average E/(Ea×Sa) indices were significantly reduced (p<0.01 for all). The baseline lateral mitral, medial mitral, and average E/(Ea×Sa) indices were significantly lower in the responder group than in the nonresponder group (p≤0.01 for all). The ROC analysis showed that all the E/(Ea×Sa) indices predict the CRT nonresponder patients. The AUC values were 0.89(lateral E/(Ea×Sa)), 0.85(average E/(Ea×Sa)), and 0.77(medial E/(Ea×Sa))(p≤0.01 for all). Conclusion:We found that the E/(Ea×Sa) index is a novel predictor of CRT nonresponder patients.