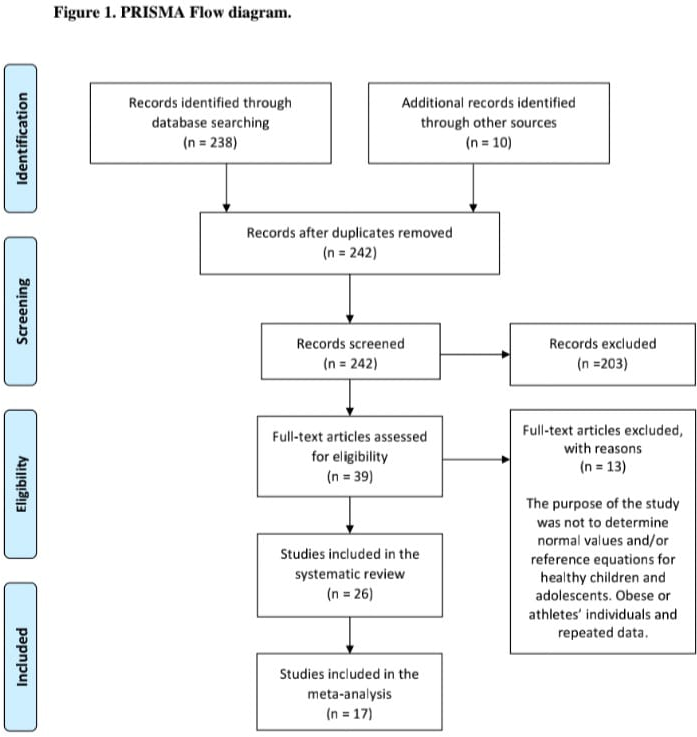
Objective: To present normative values for maximal respiratory pressures in healthy children and adolescents based on a meta-analysis of reference equations from previous publications. Data Sources: The searches were carried out until May 2020 in the following databases: ScienceDirect, Medical Literature Analysis and Retrieval System Online- MEDLINE (PubMed), Cumulative Index to Nursing and Allied Health Literature - CINAHL, Scientific Electronic Library Online - SciELO. Study Selection: Articles that determined normative values and/or reference equations for maximal inspiratory pressure (MIP) and maximal expiratory pressure (MEP) in healthy children and adolescents published in English, Portuguese, or Spanish regardless of the year of publication were included. Data Extraction: Two reviewers selected titles and abstracts to identify the studies. In case of conflict, a third reviewer was requested. Results: Initially, 248 studies were identified, 26 studies were included in the systematic review and 17 in the meta-analysis. The sample consisted of 5,190 individuals, and the MIP and MEP values were stratified by sex and age groups of 4-11 and 12-19 years. Values from 4 to 11 years for females were: 66.4 cmH2O for MIP and 74.8 cmH2O for MEP, and for males, 76.1 cmH2O for MIP and 84.7 cmH2O for MEP. In the age group from 12 to 19 years, for females were: 81.4 cmH2O for MIP and 90.1 cmH2O for MEP, and for males were 95.6 cmH2O for MIP and 108.3 cmH2O for MEP. Conclusions: This meta-analysis suggested normative values for respiratory muscle strength in children and adolescents based on 17 studies.