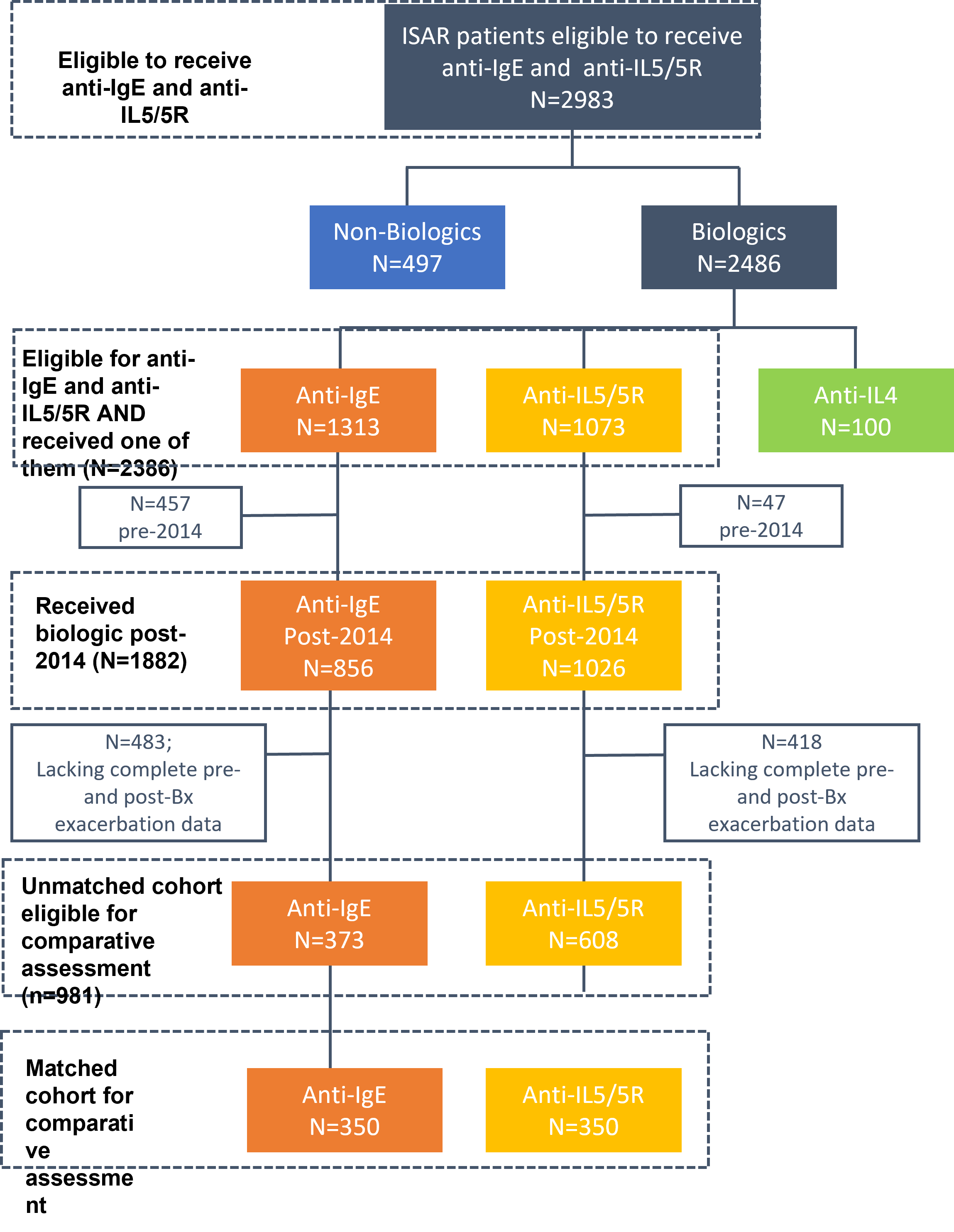
Background Patients with severe asthma may present with characteristics representing overlapping phenotypes, making them eligible for more than one class of biologic. Our aim was to describe the profile of severe adult asthma patients eligible for both anti-IgE and anti-IL5/5R and to compare the effectiveness of both classes of treatment in real life. Methods This was a prospective cohort study that included adult severe asthma patients from 22 countries enrolled into the International Severe Asthma registry (ISAR) who were eligible for both anti-IgE and anti-IL5/5R. The effectiveness of anti-IgE and anti-IL5/5R was compared in a 1:1 matched cohort. Exacerbation rate was the primary effectiveness endpoint. Secondary endpoints included long-term-oral corticosteroid (LTOCS) use, asthma-related emergency room (ER) attendance and hospital admissions. Results In the matched analysis (n=350/group), the mean annualized exacerbation rate decreased by 47.1% in the anti-IL5/5R group and 38.7% in the anti-IgE group. Patients treated with anti-IL5/5R were less likely to experience a future exacerbation (adjusted IRR 0.76; 95% CI 0.64, 0.89; p<0.001) and experienced a greater reduction in mean LTOCS dose than those treated with anti-IgE (37.44% vs 20.55% reduction; p=0.023).) There was some evidence to suggest that patients treated with anti-IL5/5R experienced fewer asthma-related hospitalizations (IRR 0.64; 95% CI 0.38, 1.08), but not ER visits (IRR 0.94, 95% CI 0.61, 1.43). Conclusions In real life, both anti-IgE and anti-IL5/5R improve asthma outcomes in patients eligible for both biologic classes, however anti-IL5/5R was superior in terms of reducing asthma exacerbations and LTOCS use.