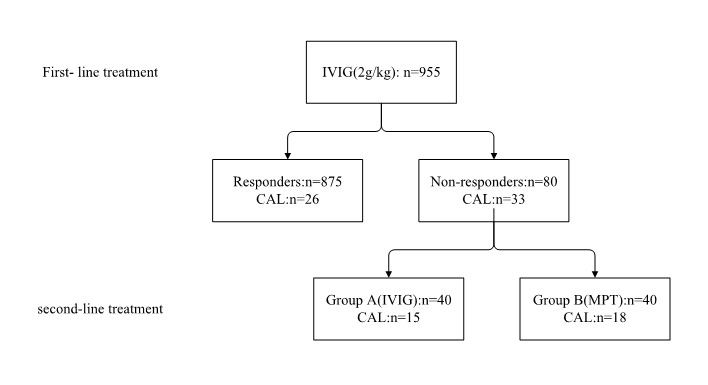
There have been no robust data from clinical trials to guide the clinician in the choice of therapeutic agents for the child with IVIG resistance, the treatment regimen for IVIG resistant patients varies between institutions, and the best option has not yet been established therefore. In this trial, a total of 955 patients with KD were selected and were initially treated with IVIG. (2g/kg), of whom 80 (8.38%) assessed as IVIG resistant were randomly divided into two groups: group A received second IVIG treatment (n = 40), group B received methylprednisolone pulse therapy (MPT, n = 40). The whole fever time, duration of fever after retreatment, hospital days, medical cost, readmission rate, and laboratory examination difference (△) were calculated. CALs outcomes were followed up over two years. Patients in MPT group had shorter fever after retreatment and lower medical costs, more rapid declines in CRP, N%, PLT levels, and more rapid rise in sodium, but had a higher incidence of treatment failure and CALs than the second IVIG treatment group in long-term follow-up. the MPT used to treat IVIG-resistant KD still need to be considered carefully.