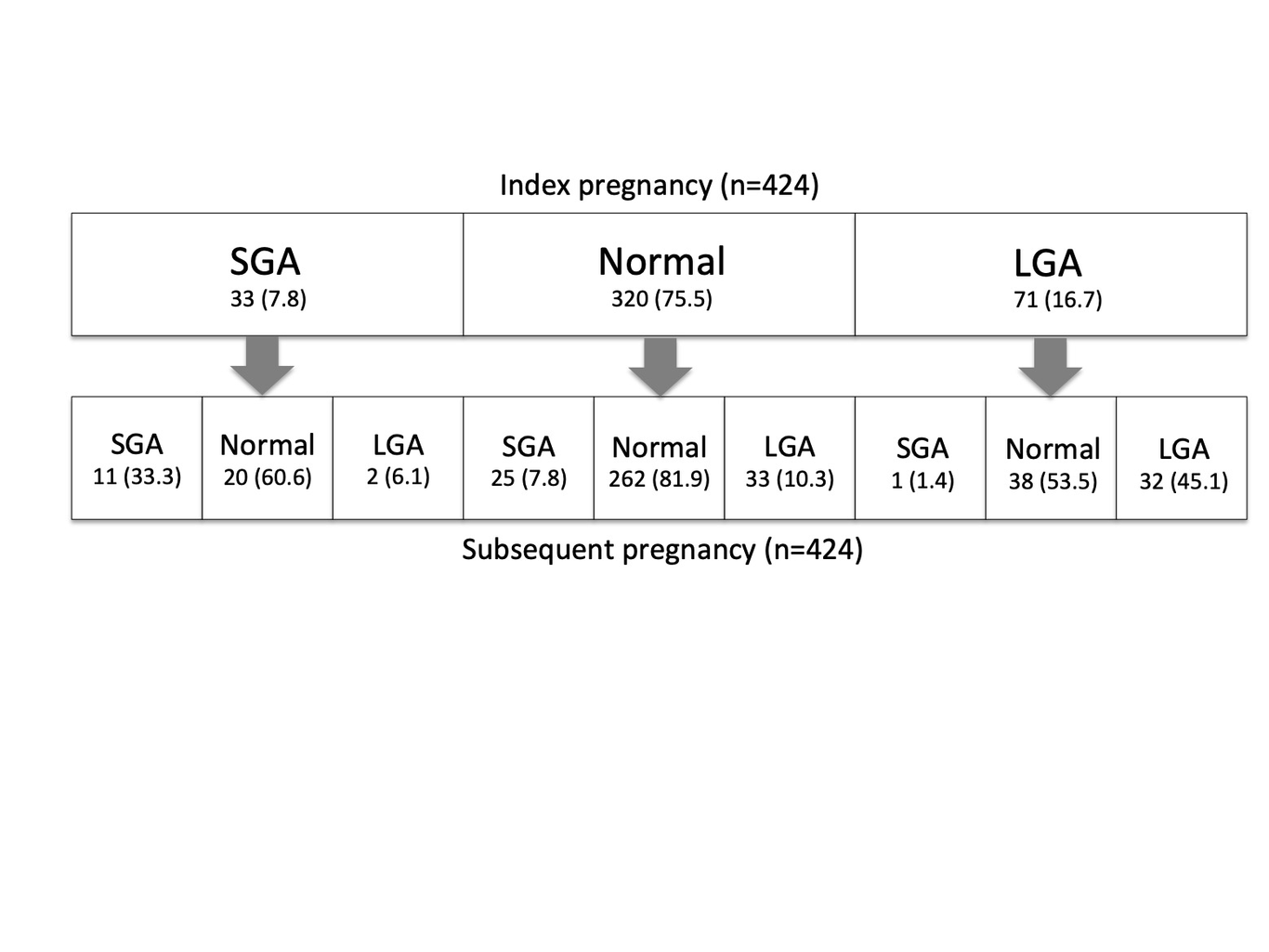
Objective: Compare the risk of recurrent adverse delivery outcome (ADO) or adverse neonatal outcome (ANO) between consecutive gestational diabetes (GDM) pregnancies. Design: Retrospective cohort Setting: Sydney, Australia Population or Sample: 424 pairs of consecutive singleton GDM pregnancies, 2003-2015 Main Outcome Measures:. ADO: instrumental delivery and emergency Caesarean. ANO: large for gestational age (LGA), small for gestational age (SGA), and composite ANO (LGA/SGA/stillbirth/neonatal death/shoulder dystocia). Methods: Using each pregnancy pair (“index” and “subsequent” pregnancy), we calculated ADO and ANO rates and determined risk factors for subsequent pregnancy outcomes (multivariate regression). Results: Subsequent pregnancies had higher rates of elective Caesarean (30.4% vs 17.0%, p<0.001) and lower rates of instrumental delivery (5% vs 13.9%, p<0.001), emergency Caesarean (7.1% vs 16.3%, p<0.001) and vaginal delivery (62.3% vs 66.3%, p=0.01). ANO rates in index and subsequent pregnancies did not differ. Index pregnancy adverse outcome was associated with a higher risk of repeat outcome: RR 3.09 (95%CI:1.30, 7.34) for instrumental delivery, RR 2.20 (95%CI:1.06, 4.61) for emergency Caesarean, RR 4.55 (95%CI:3.03, 6.82) for LGA, RR 5.01 (95%CI:2.73, 9.22) for SGA and RR 2.10 (95%CI:1.53, 2.87) for composite ANO). The greatest risk factor for subsequent LGA (RR 3.13 (95%CI:2.20, 4.47)), SGA (RR 4.71 (95%CI:2.66, 8.36)) or composite ANO (RR 2.01 (95%CI:1.46, 2.78)) was having the same outcome in the index pregnancy. Conclusions: Women with GDM and an adverse outcome are at very high risk of the same complication in their subsequent GDM pregnancy, representing a high-risk group that should be targeted for directed management over routine care.